
There is much discussion about epidurals. But what is the procedure? Which medications are used? And, how does it affect mother and baby?
The Procedure
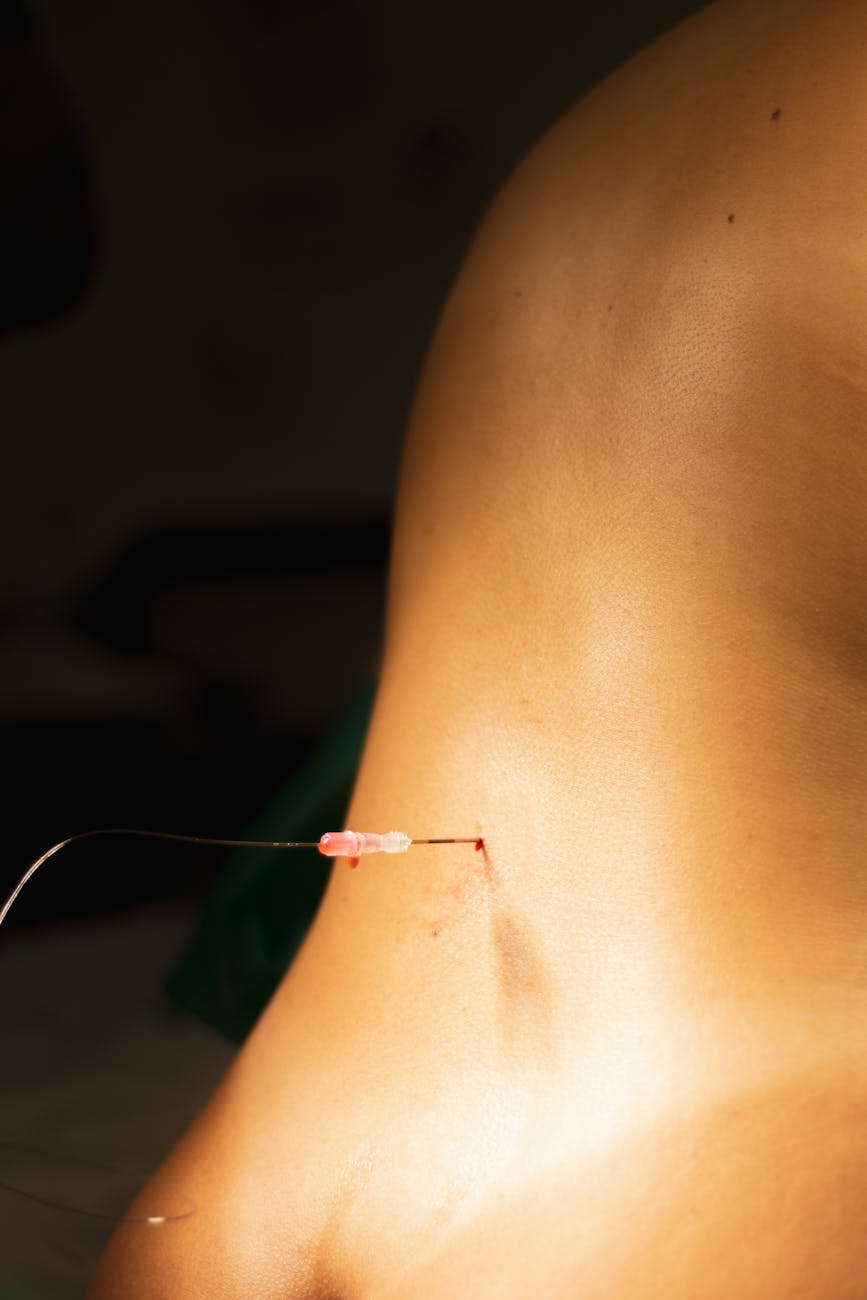
An epidural is a procedure in which a needle is inserted into the lumbar region of your vertebral column, backbone. A catheter (tube) is threaded through the needle and is placed outside your spinal cord. The catheter is taped to your back and connected to medication.
Imagine your spinal cord is a set of electrical wires wrapped by a rubber encasing called the dura mater. The epidural is placed outside the dura mater; hence, the name epi-dural.
In contrast, a spinal block goes past the dura mater, into the same space as your spinal cord. Spinal blocks are used for c-sections. It is less common to use a spinal for vaginal birth. But, a spinal may be combined with an epidural in labor for both immediate and continuous pain relief, respectively.
Placing an epidural is a sterile procedure. Your family will be asked to leave the room. This is to reduce the risk of the birthing person developing an infection of the nervous system.
The Meds
Anesthetics and analgesics are the medications used to treat discomfort during labor and delivery. Analgesics are pain relievers. Anesthetics can reduce sensation all together. Most of the medications used in epidurals are anesthetics known in medicine as caine drugs. Lidocaine, which can be found over the counter (OTC) in lower doses, is an example of a caine drug. They may be given alone or with opioids. The most common epidural ‘cocktail’ I have seen in Labor & Delivery is Bupivacaine with Fentanyl.
The medication given in an epidural may be continuous or intermittent. Continuous means the birthing person is receiving a continuous flow of medication. Intermittent means the birthing person is receiving doses of medication at programmed intervals of time, for example every 45 minutes. In addition, the patient may be given patient-controlled analgesia (PCA), a button to push when pain is felt. This is sometimes referred to as a bolus. A bolus also can be given by the anesthetist. My observation as a doula has been that birthing persons who take boluses deliver babies that appear less awake and need a higher level of pediatric care; a difficult second stage (delivery) may be a contributing factor.
Research suggests intermittent epidurals have better pain relief outcomes than continuous. But bias was found high and/or of concern in a meta-analysis of the research done around the specifics of intermittent programmed epidural bolus (IPB) use. A meta-analysis analyzes all of the research done on a subject.
Effects on Mother and Baby
Epidurals can cause itching, fever, headaches, back pain, and low blood pressure in mothers. Less commonly, epidurals can cause life-threatening infection or leaking of spinal fluid.
For the most part, the research is inconsistent regarding the effects of epidurals on newborns. Researchers will say opioids used in an epidural reduce the breathing, muscle tone, and alertness of a newborn but then that the APGAR scores, which measure these outcomes, are unaffected. The same goes for breastfeeding. A baby’s exposure to an epidural opioid is minuscule compared to systemic opioid use. It is unlikely that a newborn will experience withdrawal or seizures after exposure from an epidural opioid. That being said, in my experience as a doula, newborns who were exposed to epidurals have a harder time with the coordination necessary for breastfeeding than newborns delivered naturally.
Epidurals are associated with higher rates of instrumental births – births using forceps or vacuums. Forceps births can cause facial paralysis. Facial paralysis may resolve on its own, respond to treatment, or become permanent usually to one side of the jaw. An uneven cry or eyelid that will not shut is a sign of facial paralysis.
Epidurals are associated with higher rates of neonatal resuscitation and Neonatal Intensive Care Unit (NICU) admissions but not with childhood developmental delays at 2 years old. An epidural at childbirth may be a protective factor in communication and fine motor skills at 2 years old.
Alternatives to Epidurals
Doula comfort measures, showers, nitrous oxide, Tylenol, hypnobirth, and TENS are all alternatives to using an epidural. Having a realistic expectation of discomfort during labor & delivery may de-catastrophize the experience. An average 7lb newborn is coming out of the human body. To expect a 0 on the pain scale is not realistic. Setting a realistic expectation and reminding everyone involved that childbirth is normal may reduce fear, tension, and pain.
References
- What to Know About Epidurals and Epidural Side Effects (parents.com)
- Meninges: What They Are & Function (clevelandclinic.org)
- Birth: Learn More – Epidurals and other medications to relieve labor pain – InformedHealth.org – NCBI Bookshelf
- Medications for Pain Relief During Labor and Delivery | ACOG
- ASHP-PCA-and-Epidural-Standards.pdf
- Intermittent epidural bolus versus continuous epidural infusions for labor analgesia: A meta-analysis of randomized controlled trials – PMC
- Influence of different volumes and frequency of programmed intermittent epidural bolus in labor on maternal and neonatal outcomes: A systematic review and network meta-analysis – PubMed
- Side effects of an epidural – NHS (www.nhs.uk)
- Association of Epidural Analgesia in Women in Labor With Neonatal and Childhood Outcomes in a Population Cohort | Anesthesiology | JAMA Network Open | JAMA Network
- Facial nerve palsy due to birth trauma: MedlinePlus Medical Encyclopedia
- Epidurals During Childbirth: What Women Should Know > News > Yale Medicine
- Is Tylenol Safe During Pregnancy?
